I. Introduction: The Evolution of Venous Access
The Shift in Medical Care
The landscape of modern vascular access has undergone a profound transformation over the last century. Early intravenous therapies relied exclusively on rigid steel needles, which, while effective for immediate puncture, posed severe risks for continuous use. If a patient moved, the unyielding steel could easily puncture the posterior wall of the vein, leading to rapid infiltration, hematomas, and severe patient discomfort.
The most significant leap in vascular therapy was the development of the внутривенная игла, commonly referred to today as the peripheral IV. By introducing a flexible catheter over a sharp introducer needle, medical professionals could perform the initial venipuncture with precision, retract the sharp steel, and leave only a soft, pliable tube within the vascular system. This innovation drastically improved patient comfort, extended the dwell time of the access site, and practically eliminated the risk of mechanical vein perforation during patient movement.
Manufacturer’s Perspective
From a manufacturing and global supply chain perspective, producing a high-quality intravenous IV cannula requires absolute precision. As global healthcare infrastructure expands, so does the demand for zero-defect medical consumables. Leading manufacturers operate under strict ISO 13485 quality management systems, utilizing Class 100,000 cleanrooms to ensure that every component is free from particulate contamination and pyrogens.
For hospital procurement teams, medical device distributors, and B2B buyers, understanding the engineering behind these devices is critical. Selecting the right manufacturer means ensuring that the catheter material, needle bevel geometry, and safety mechanisms are flawlessly executed. A failure in manufacturing—such as a poorly adhered catheter tip or a dull introducer needle—can lead to immediate clinical failure, compromising patient safety and escalating healthcare costs.
II. Anatomy of a Modern IV Cannula
To fully grasp the differences in clinical application, buyers must first understand the structural anatomy of these devices. Every component is engineered to balance ease of insertion with long-term biocompatibility.
The Catheter Material
The defining feature of modern intravenous access is the plastic IV cannula. Historically, materials like PVC were used, but modern manufacturing has transitioned almost exclusively to two premium polymers:
- FEP (Fluorinated Ethylene Propylene): Also known as Teflon, FEP is highly lubricious. It offers an exceptionally smooth surface, which reduces friction during insertion and minimizes the risk of mechanical phlebitis. FEP catheters are relatively firm, making them easier to advance through tough skin.
- PUR (Polyurethane): PUR is highly thermo-sensitive. While it is firm at room temperature (aiding in insertion), it softens significantly once exposed to body heat. This softening allows the catheter to float comfortably within the vein, reducing irritation to the endothelial lining and allowing for longer dwell times.
Terminology Clarification
In the medical supply industry, buyers frequently encounter the terms IV cannula and IV catheter. While they are often used interchangeably on the hospital floor, technically, the “cannula” refers to the entire assembled device (including the needle, hub, and flashback chamber), whereas the “catheter” strictly refers to the flexible plastic tube that remains in the patient’s vein.
Structural Components
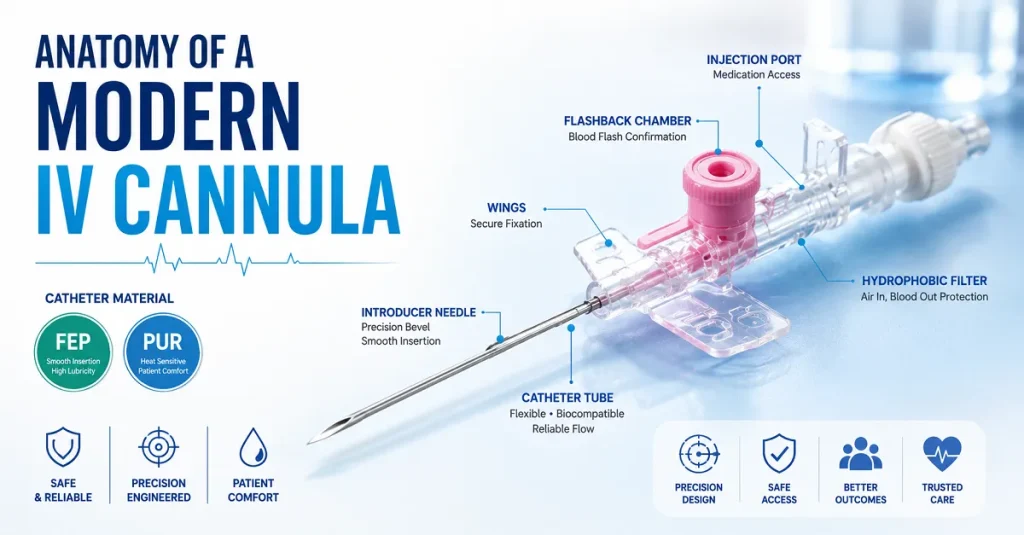
A premium cannula consists of several highly engineered parts:
- The Introducer Needle: Manufactured from surgical-grade stainless steel (usually SUS304), the needle features a micro-precision back-cut bevel. This specific geometry creates a V-shaped incision in the tissue rather than a core puncture, reducing insertion pain and promoting faster tissue healing upon removal.
- The Tube: Сайт IV cannula tube undergoes a precise extrusion process. The tip must be meticulously tapered to adhere flush against the steel needle, ensuring a seamless transition that prevents the plastic from peeling back (the “accordion effect”) upon entering the skin.
- The Injection Port: Found on specific models, the IV cannula injection port features a one-way silicone valve. This allows nurses to administer direct bolus medications via a syringe without interrupting the primary continuous fluid line, all while preventing backflow of blood.
- Flashback Chamber and Hydrophobic Filter: Located at the rear hub, this clear chamber allows the clinician to instantly confirm successful vein entry when blood “flashes” back. A microscopic hydrophobic filter allows air to escape the chamber so blood can enter, but strictly prevents blood from spilling out.
III. Categorizing Different Types of IV Needles
Global markets demand variations in design to accommodate different healthcare protocols, regional preferences, and specific patient anatomies. Understanding the different types of IV needles is essential for medical distributors curating their product portfolios.
Ported vs. Non-Ported Models
Стандарт type cannula varies primarily based on the presence of an injection port and fixation wings.
- Pen-Type (Straight) Cannula: This design lacks wings and an injection port, resembling a standard pen. It is highly favored in regions where cost-efficiency is paramount and for quick, straightforward fluid administration. Its low profile makes it less likely to catch on clothing or bedding.
- Ported Cannula with Wings: This is the most common model globally. The butterfly-style wings allow for secure taping to the patient’s skin, reducing mechanical dislodgement. The top injection port provides immediate access for emergency drugs.
Advanced Safety Designs
With strict occupational health regulations globally (such as OSHA in the United States), there is a massive shift toward the needleless shielded cannula, commonly known as a Safety IV Cannula. Needlestick injuries pose a severe risk of transmitting bloodborne pathogens like HIV and Hepatitis to healthcare workers.
- Passive Safety Mechanisms: As the clinician retracts the steel needle from the catheter hub, a metal or plastic clip automatically snaps over the sharp bevel. This requires no extra steps from the user, ensuring 100% compliance.
- Active Safety Mechanisms: The user must manually push a button or slide a sheath to cover the needle.
Pediatric and Neonatal Care
Manufacturing a Pedia IV cannula requires the highest level of precision. Neonatal veins are incredibly fragile and tiny. These devices (typically 24G or 26G) require ultra-thin-walled catheter extrusion to maximize the internal flow rate while keeping the outer diameter as small as possible. The needles undergo additional electropolishing to ensure absolute smoothness for the most delicate venipuncture.
Multi-Directional Access
For complex clinical scenarios, such as the ICU or operating theater, buyers often inquire about 3-way IV cannula uses. While a standard cannula provides a single access point, they are frequently connected to 3-way stopcock valves. This setup allows for the simultaneous administration of multiple fluids—for instance, running continuous saline hydration while concurrently pushing a localized antibiotic, all controlled by turning the stopcock valve without needing a second venipuncture.

IV. IV Cannula Types and Sizes: The Global Gauge System
The core of vascular access procurement relies on understanding the standardized ISO color-coding system. This system ensures that a nurse in Germany and a doctor in Brazil can instantly identify the size of the catheter by the color of its hub.
When evaluating IV cannula types and sizes, the general rule dictated by Poiseuille’s Law of fluid dynamics applies: flow rate is proportional to the radius to the fourth power. Therefore, a slight increase in the catheter’s internal diameter yields a massive increase in flow rate. Conversely, the gauge (G) number is inversely proportional to the diameter—the lower the gauge number, the thicker the needle.
Below is an authoritative breakdown of IV cannula types and uses, detailing the specifications necessary for B2B procurement decisions.
Comprehensive Guide to Gauges and Flow Rates
| Манометр (G) | Цвет концентратора ISO | Внешний диаметр (мм) | Avg. Flow Rate (ml/min) | Основное клиническое применение |
| 14G | Оранжевый | 2,10 мм | 240 – 270 ml/min | Massive trauma, operating theater, rapid volume replacement. |
| 16G | Серый | 1.80 mm | 180 – 200 ml/min | Major surgeries, rapid blood transfusions, severe dehydration. |
| 17G | Белый | 1.50 mm | 130 – 140 ml/min | Specialized blood donation, veterinary medicine (less common in standard human wards). |
| 18G | Зеленый | 1.30 mm | 90 – 100 ml/min | Standard for blood transfusions, CT contrast injection, and major surgery preparation. |
| 20G | Розовый | 1.10 mm | 60 – 65 ml/min | The universal standard for routine peripheral iv cannulation, routine fluids, and antibiotics. |
| 22G | Голубой | 0,90 мм | 36 – 40 ml/min | Older adults, pediatric patients, patients with difficult or fragile veins, prolonged antibiotic therapy. |
| 24G | Желтый | 0,70 мм | 20 – 23 ml/min | Neonates, infants, oncology patients with severely compromised vascular systems. |
| 26G | Violet | 0,60 мм | 13 – 15 ml/min | Premature neonates, highly specialized micro-infusions. |
Deep Dive into Clinical Uses
14G (Orange) & 16G (Grey): The Trauma Lifesavers. These are massive catheters used almost exclusively in emergency departments, operating rooms, and by paramedics. When a patient is experiencing hypovolemic shock (massive blood loss), rapid fluid resuscitation is the difference between life and death. A 14-G catheter can empty a 1-liter bag of saline in under four minutes. Inserting these requires a large, healthy vein, typically in the antecubital fossa (the crook of the arm).
18G (Green): The Transfusion Standard Blood is a viscous fluid containing fragile red blood cells. If forced through a narrow catheter, the cells can shear and rupture (hemolysis). Therefore, an 18-G is the minimum standard for rapid, safe blood transfusions. It is also required for high-pressure injection of radiopaque contrast media during CT scans.
20G (Pink): The Universal Workhorse. If a hospital could only stock one size, it would be the 20G. It provides the perfect balance: the needle is small enough to comfortably fit into most adult veins on the forearm or back of the hand, yet the internal diameter is wide enough to support routine hydration, push medications, and even slow blood transfusions if an 18G cannot be placed.
22G (Blue): The Gentle Alternative. As patients age, their veins lose elasticity, becoming fragile and prone to blowing (rupturing) during insertion. The 22G is the standard choice for geriatric populations. It is also the preferred size for patients requiring long-term, slow-drip antibiotic therapy where a high flow rate is unnecessary, but preserving the vein’s integrity for days is crucial.
24G (Yellow) & 26G (Violet): Precision Neonatal Care. These represent the pinnacle of extrusion technology. Used primarily as a pedia IV cannula, these sizes are inserted into the tiny veins of infants’ scalps, hands, or feet. Because the flow rate is so low (15-20 ml/min), they are strictly used with infusion pumps that precisely control the micro-drip delivery of medications and nutrition to premature babies.

V. B2B Sourcing: Factors Influencing IV Cannula Price
For medical distributors and hospital procurement departments, understanding the variables that determine IV cannula prices is essential for optimizing supply chains without compromising clinical safety. The manufacturing of medical consumables operates on tight margins, and several highly technical factors drive price fluctuations.
1. Raw Material Selection
The choice between FEP (Teflon) and PUR (Polyurethane) for the IV cannula catheter significantly impacts the cost. PUR is inherently more expensive to source and process than FEP. However, because PUR softens in the vein, it dramatically reduces the rate of phlebitis. Hospitals often find that paying a slight premium for PUR catheters saves money overall by reducing the number of cannula restarts required per patient.
2. Needle Geometry and Processing
Standard bevels are relatively inexpensive to grind. However, premium manufacturers utilize a multi-faceted, ultrasonic back-cut grinding process, followed by an electro-polishing phase and a micro-siliconization coating. This ensures the needle glides through tissue with microscopic friction. Cutting corners on needle grinding lowers the price but drastically increases patient pain and insertion failure rates.
3. Safety Mechanisms
The integration of a needleless shielded cannula mechanism inherently drives up the unit cost due to the additional plastic/metal components and complex automated assembly required. However, in regions like the US and EU, safety cannulas are legally mandated. Furthermore, the cost of treating a single hospital-acquired needlestick injury (which can run into tens of thousands of dollars) far outweighs the pennies-per-unit premium of a safety cannula.
4. Cleanroom and Sterilization Standards
Authentic medical manufacturing requires massive overhead to maintain Class 100,000 (ISO 8) cleanrooms. Furthermore, the preferred method of sterilization for these devices is Ethylene Oxide (EtO) gas. The EtO process requires strict temperature and humidity controls, followed by a lengthy degassing quarantine period to ensure no toxic gas residue remains on the plastic. Manufacturers offering prices that seem “too good to be true” often cut corners on cleanroom maintenance or shorten the critical degassing phase, risking patient safety and regulatory action.
5. Automated Visual Inspection (AVI)
The highest-tier factories do not rely solely on human visual inspection. They employ high-speed camera systems driven by AI to inspect the catheter tip for microscopic burrs or flash, ensuring the needle bevel aligns perfectly with the catheter. This machinery requires heavy capital investment but guarantees a zero-defect batch, protecting the buyer’s brand reputation.

VI. Часто задаваемые вопросы (Q&A)
To further assist buyers and clinical users in understanding the types of IV cannula and their uses, we have compiled the most critical industry queries.
Historically, guidelines from organizations like the CDC recommended routinely replacing a peripheral IV cannula every 72 to 96 hours to prevent infection. However, modern clinical practice and updated guidelines now advocate for “clinically indicated replacement.” This means that as long as the insertion site shows no signs of complications (redness, swelling, pain) and the cannula remains fully functional, it can be left in place, provided it is rigorously assessed by nursing staff every single shift.
While generally very safe, the primary risks involve localized vascular complications. The most common is phlebitis (mechanical or chemical inflammation of the vein). Infiltration occurs if the catheter slips out of the vein, causing IV fluids to pool in the surrounding tissue. In severe cases, poor sterile technique during insertion can lead to localized infections or, rarely, systemic bloodstream infections.
A traditional steel needle is rigid. If a patient bends their arm or moves unexpectedly while a steel needle is taped in their vein, the sharp tip will easily lacerate the vein wall, causing bleeding and ruining the access site. An внутривенная игла mitigates this by completely removing the steel introducer once access is achieved. It leaves behind only a soft, flexible plastic IV cannula that bends and moves with the patient’s anatomy, causing zero internal damage.
Intravenous access is broadly categorized by where the catheter tip terminates:
Peripheral IV Cannulation: The most common, placed in small veins of the hand or arm for short-term use.
Midline Catheters: Longer catheters inserted in the upper arm, terminating before the shoulder, used for intermediate therapies (1-4 weeks).
Central Venous Catheters (CVC): Inserted into large veins (neck, chest, or groin) with the tip resting near the heart, used for highly concentrated drugs and critical care.
To maintain the patency (openness) of the IV cannula tube, standard hospital protocol requires flushing the line with 2 to 5 mL of sterile normal saline. This must be done immediately before and after administering any medication to clear the line. If the cannula is “locked” (not currently attached to a continuous drip), it should be flushed at least once every 8 to 12 hours to prevent blood from coagulating and blocking the plastic tube.
Insertion requires strict aseptic technique. The clinician applies a tourniquet to engorge the vein, cleans the skin with chlorhexidine, and anchors the vein. The introducer needle and catheter are inserted at a 10-to-30-degree angle. Once a “flash” of blood is seen in the chamber, the angle is lowered, the catheter is advanced fully into the vein over the needle, the tourniquet is released, and the steel needle is fully retracted and safely discarded.
The insertion process causes a brief, sharp pinch as the steel needle breaches the skin and vein wall. However, because premium manufacturers utilize high-precision back-cut bevels and micro-siliconization, this pain is minimized and lasts only a few seconds. Once the needle is removed and only the soft plastic catheter remains, the patient should feel absolutely no pain during rest or fluid administration.
A ported cannula includes an integrated secondary injection port located on top of the device, equipped with a one-way valve. This allows nurses to instantly push emergency drugs or saline flushes directly into the vein without having to disconnect the primary IV fluid line. A non-ported (pen-style) cannula lacks this feature, requiring all medications to be administered through the primary line’s connection hub, making it slightly less versatile but more cost-effective.


