I. Introduction: The Frontline of Diagnostic Precision
In the modern landscape of oncology, pathology, and interventional radiology, diagnostic accuracy is the undisputed cornerstone of effective patient care. Before a surgical intervention is planned or a targeted chemotherapy regimen is prescribed, clinicians rely on the definitive answers provided by tissue and cellular analysis. At the absolute center of this diagnostic pathway is a highly engineered medical consumable: the биопсийная игла.
The ongoing clinical discussion regarding core needle biopsy vs fine needle aspiration (FNAC) is not merely an academic debate; it is a practical, daily decision made by physicians worldwide. Selecting the correct modality—and by extension, the correct instrument—dictates the quality of the sample, the comfort of the patient, and the speed of the diagnosis.
As a dedicated manufacturer of premium medical consumables, we recognize that producing a biopsy needle requires an uncompromising commitment to precision engineering. A needle must be sharp enough to penetrate dense fibrotic tissue without causing trauma, yet structured enough to capture an intact tissue sample. From the surgical-grade stainless steel cannula to the laser-etched echogenic tips designed for flawless ultrasound visibility, every millimeter of the instrument serves a critical purpose.
This comprehensive guide delves into the mechanical, clinical, and procurement aspects of biopsy instruments. By detailing the specific requirements across different anatomical targets, we aim to equip medical distributors, pharmacy buyers, and hospital procurement networks with the authoritative knowledge necessary to optimize their diagnostic supply chains.
II. Understanding the Modalities: Aspiration vs. Core Techniques
To supply a hospital network effectively, procurement officers must understand the fundamental differences between the two primary tissue sampling techniques. While both involve inserting a needle into a suspicious lesion, the physics, the instruments, and the laboratory processing pathways are entirely distinct.
A. Fine Needle Aspiration Cytology (FNAC)
When clinicians and patients ask what needle aspiration biopsy is, they are inquiring about the least invasive tissue sampling method available in modern medicine.
- The Clinical Definition: Fine Needle Aspiration Cytology (FNAC) is a diagnostic procedure utilized to investigate lumps or masses. Unlike techniques that remove chunks of tissue, FNAC extracts individual cells, cell clusters, and fluid from the lesion. These cells are smeared onto a glass slide, stained, and examined by a cytopathologist.
- The Instrument: A fine aspiration needle biopsy utilizes ultra-fine needles, typically ranging from 22G to 27G. The procedure relies on the physics of a vacuum. The needle is attached to a syringe (often held in a specialized syringe pistol grip for one-handed operation). Once the needle enters the lesion, the practitioner pulls back on the plunger, creating negative pressure. Through rapid, microscopic forward-and-backward motions within the mass, capillary action and the vacuum draw loose cells into the needle hub.
- Преимущества: FNAC is remarkably fast, virtually painless (often requiring no local anesthesia), and boasts a highly rapid turnaround time for lab results. It is the gold standard for evaluating fluid-filled cysts and highly cellular superficial nodules.
B. Core Needle Biopsy (CNB)
For many modern diagnostic protocols, particularly in breast and prostate oncology, cytology (examining individual cells) is no longer sufficient. Pathologists need histology—the examination of the cells within their structural and architectural context. This answers the question: What is a core needle biopsy?
- The Clinical Definition: A core needle biopsy is a procedure designed to extract an intact, solid cylinder (or “core”) of tissue from a tumor. By preserving the tissue’s stroma and cellular architecture, pathologists can accurately grade tumors, differentiate between in-situ and invasive carcinomas, and perform vital immunohistochemical (IHC) staining to identify specific hormone receptors (like HER2 in breast cancer).
- The Instrument: Core biopsy needles are robust instruments, typically ranging from 14G to 18G. They are mechanically complex, featuring a two-part system: an inner solid stylet with a specialized “sample notch” (a cutout where the tissue rests) and an outer, razor-sharp cutting cannula.
- The Mechanism: The needle is advanced to the tumor. The inner stylet is thrust forward into the mass, allowing tissue to prolapse (fall) into the sample notch. Instantly, the outer cutting cannula fires forward over the stylet, slicing the tissue clean and trapping the intact core safely inside the notch for extraction.
Table 1: Comparative Analysis – FNAC vs. Core Needle Biopsy
| Характеристика | Fine Needle Aspiration (FNAC) | Core Needle Biopsy (CNB) |
| Тип образца | Individual cells and fluid (Cytology) | Intact tissue cylinder (Histology) |
| Игольчатый калибр | 22G – 27G (Very Thin) | 14G – 18G (Thick) |
| Anesthesia | Often not required | Local anesthesia strictly required |
| Механизм | Vacuum suction / Capillary action | Mechanical slicing / Shearing |
| Primary Use Cases | Thyroid, Lymph nodes, Cysts, Salivary | Breast, Liver, Kidney, Prostate, Lungs |
| Complication Risk | Extremely Low | Low to Moderate (Bleeding risk) |
| Diagnostic Yield | Good for initial screening | Local anesthesia is strictly required |
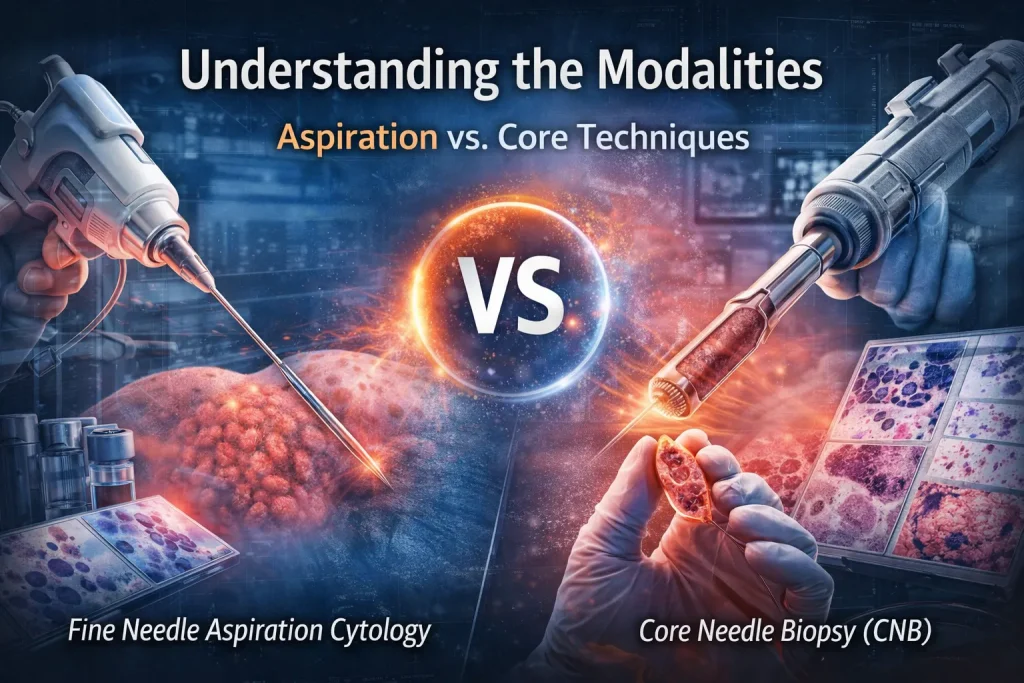
III. Product Showcase: Types of Biopsy Needles by Anatomy
The human body presents a diverse array of anatomical challenges. A needle designed to sample a superficial lymph node will fail disastrously if used to sample a deep, mobile kidney. As a manufacturer, our portfolio of various types of biopsy needles is categorized by the target organ system, each engineered with distinct safety and efficacy features.
A. Superficial and Glandular Biopsies
Superficial glands are often highly vascular and located near critical structures (like the carotid artery or the trachea). Precision and visibility are paramount.
- Thyroid Diagnostics: A Fine needle biopsy of thyroid nodules is the definitive test for ruling out thyroid cancer. Because the thyroid is small and situated in the neck, this procedure is almost universally performed under ultrasound guidance. Needles manufactured for this purpose feature “echogenic tips.” We utilize microscopic laser dimpling on the final centimeters of the needle shaft. These dimples reflect ultrasound waves brightly back to the transducer, ensuring the physician can see the exact location of the needle tip in real-time, avoiding the jugular vein.
- Lymphatic System and Head/Neck: When investigating adenopathy, a lymph node needle biopsy is frequently deployed. The neck biopsy needle must be agile. Because lymph nodes can be tough and rubbery, we manufacture these fine needles with an ultra-sharp, multi-beveled trocar tip to prevent the needle from simply pushing the node aside (a phenomenon known as “tenting”).
- Breast Oncology: Сайт breast biopsy needle is perhaps the most heavily utilized core needle in the world. Mammography and ultrasound identify lesions, but the needle confirms the pathology. Standard breast core biopsies use a 14-G spring-loaded automated gun. However, for microcalcifications, clinicians use Vacuum-Assisted Biopsy (VAB) probes (often 9G to 11G). These large, motorized needles use a vacuum to continuously suck tissue into a rotating cutting chamber, allowing the physician to remove multiple large samples—or even entirely excise a small benign fibroadenoma—with a single needle insertion.
B. Deep Tissue and Abdominal Biopsies
Abdominal organs are highly vascularized and often move with the patient’s respiration, requiring specialized designs to prevent internal hemorrhage.
- Hepatic Interventions: The liver filters blood, making a Liver biopsy needle design an exercise in risk mitigation. Historically, the Menghini needle (a suction-based core needle) was used. Today, semi-automatic Tru-cut style needles (16G or 18G) are preferred. Our liver needles are designed with a specifically calibrated “throw length” (the distance the cutting cannula travels). By offering short-throw options (e.g., 10mm instead of 22mm), we reduce the risk of the needle passing completely through the liver capsule and causing a catastrophic bleed.
- Renal Diagnostics: A needle biopsy of the kidney is essential for diagnosing medical renal diseases (like glomerulonephritis) and staging renal cell carcinoma. Kidneys are located deep in the retroperitoneum. Renal biopsy needles often feature coaxial introducer systems. A shorter, wider guide needle (the coaxial) is inserted first, stopping just short of the kidney. The actual biopsy needle is then passed through this guide tube multiple times to obtain several cores without having to repeatedly puncture the skin and surrounding muscle fascia.
- Gastrointestinal and Pancreatic: A percutaneous approach (through the skin) is often too dangerous for a needle biopsy of the pancreas due to the surrounding stomach and bowel. Instead, Endoscopic Ultrasound (EUS) is used. The needle is passed down an endoscope into the stomach and pushed directly through the stomach wall into the adjacent pancreas. These needles (EUS-FNA or EUS-FNB) must be incredibly long and made from Nitinol (a nickel-titanium alloy) rather than standard steel, providing extreme flexibility to navigate the curved channels of the endoscope without permanently kinking.
C. Thoracic, Dermatological, and Orthopedic Specialties
- Respiratory System: A trans-thoracic lung biopsy needle is used to sample pulmonary nodules. The primary risk here is pneumothorax (lung collapse) caused by air leaking into the chest cavity. Our lung biopsy systems utilize a specialized coaxial needle with an airtight hemostatic valve. This allows the inner biopsy needle to be removed while the outer guide cannula remains sealed, preventing air from rushing into the pleural space.
- Dermatology: Unlike deep organs, skin lesions require full-thickness sampling of the epidermis, dermis, and subcutaneous fat. The punch needle biopsy resembles a tiny, circular cookie cutter (ranging from 2mm to 8mm in diameter). The physician rotates the sharp hollow blade downward into the skin, extracting a perfect cylindrical plug of tissue for the diagnosis of melanomas or inflammatory dermatoses.
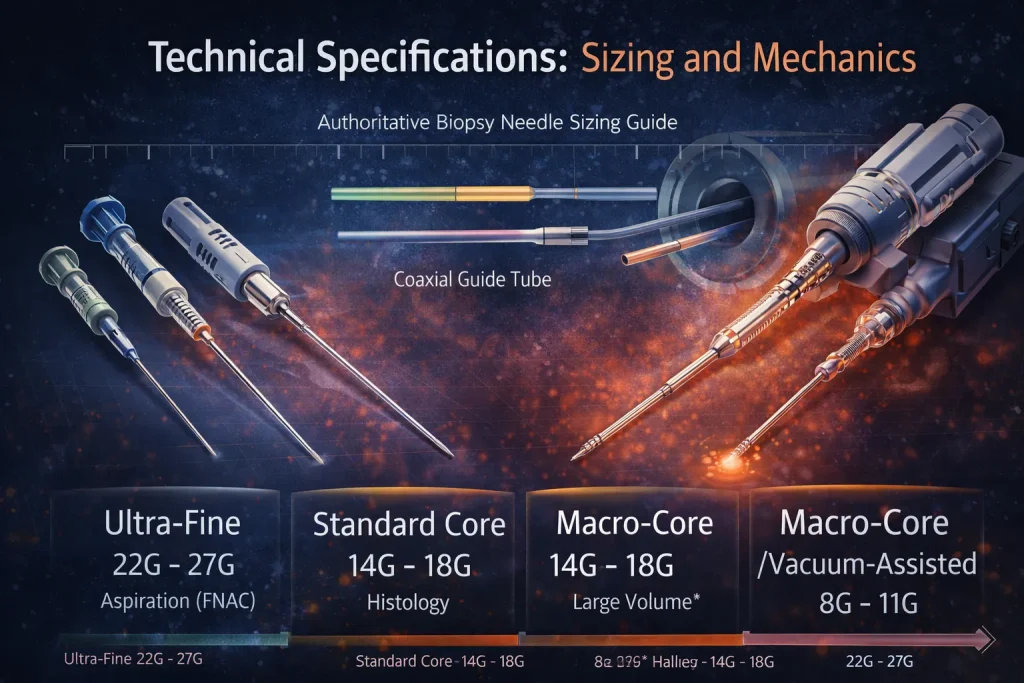
IV. Technical Specifications: Sizing and Mechanics
For hospital procurement officers and interventional radiologists, understanding the exact technical specifications of biopsy instruments ensures that the right tool is available in the surgical suite.
A. The Gauge System in Biopsy
The medical industry utilizes the Birmingham Wire Gauge (BWG) system to categorize the size of biopsy needles. It is an inverse scale: the lower the gauge number, the larger the outer diameter of the needle.
- Ultra-Fine (22G – 27G): Used exclusively for aspiration (FNAC). They cause minimal trauma.
- Standard Core (14G – 18G): The workhorses of the histology department. An 18G is standard for the prostate and liver; a 14G is standard for the breast.
- Macro-Core / Vacuum Assisted (8G – 11G): Used for removing massive volumes of tissue, particularly in breast oncology and bone marrow extraction.
Table 2: Authoritative Biopsy Needle Sizing Guide
| Манометр (G) | Внешний диаметр (мм) | Primary Modality | Standard Anatomical Target |
| 8G – 11G | 3.4mm – 3.0mm | Vacuum-Assisted / Bone | Breast Microcalcifications, Iliac Crest (Bone) |
| 14G | 2.1mm | Биопсия с помощью иглы | Breast Tumors, Soft Tissue Sarcomas |
| 16G | 1.6mm | Биопсия с помощью иглы | Kidney, Transplant evaluation, Liver nodules |
| 18G | 1.2mm | Биопсия с помощью иглы | Prostate, Liver, Lung |
| 20G | 0.9mm | Core / Aspiration | Thyroid core, specialized lung |
| 22G | 0.7mm | Fine Needle Aspiration | Thyroid nodules, Superficial Lymph Nodes |
| 25G | 0.5mm | Fine Needle Aspiration | Pediatric nodes, delicate facial cysts |
B. Orthopedic Specifications: Bone Marrow
Hematological cancers (like leukemia or lymphoma) require sampling the spongy tissue inside large bones. The bone marrow biopsy needle size is typically massive, ranging from 8G to 13G (for pediatrics).
Because the physician must manually push and twist the needle through the hard, calcified outer cortex of the posterior iliac crest (pelvis), the needle must possess immense structural integrity to prevent snapping. These needles (often modeled on the classic Jamshidi design) feature specialized ergonomic, T-shaped or bulbous handles that distribute the physician’s applied pressure evenly across the palm, preventing hand fatigue during the difficult extraction process.
C. Mechanical Innovations: From History to Automation
The evolution of biopsy tools is a study in mechanical engineering. Clinicians occasionally ask what a Silverman biopsy needle is used for. Developed in the 1930s, the Silverman needle was one of the first true core biopsy instruments. It featured a longitudinally split inner stylet. The physician would manually push the split stylet into the tissue, and the prongs would grasp the tumor.
While revolutionary for its time, manual needles like the Silverman were highly dependent on the physician’s speed and physical strength. A slow thrust would merely push the tumor away.
Today, the Silverman has been entirely replaced by spring-loaded, automated biopsy guns. These modern devices use heavy-duty internal springs. With the press of a button, the stylet and cutting cannula fire in a fraction of a second (often under 20 milliseconds). This high-velocity firing cleanly shears the tissue before the tumor has a chance to move, resulting in vastly superior sample quality and significantly less pain for the patient.
V. Procurement and Supply Chain Solutions
For B2B buyers and medical distributors, the clinical efficacy of a needle is only relevant if the supply chain is impenetrable. A shortage of biopsy needles directly delays cancer diagnoses, halting patient treatment plans.
A. Original Equipment Manufacturing (OEM) and Bulk Supply
As a premier manufacturer, we specialize in supplying large-scale hospital networks and global medical distributors. We offer comprehensive OEM services, allowing distributors to private-label our precision-engineered needles. Our manufacturing facilities are equipped to scale production seamlessly, ensuring that high-volume items—such as 14G breast core needles and 22G thyroid aspiration needles—are never backordered.
B. Uncompromising Quality Assurance and Sterilization
Biopsy needles are introduced deep into sterile body cavities. An infection introduced via a contaminated needle can be fatal.
- ISO 13485 Compliance: Our entire manufacturing ecosystem operates under strict ISO 13485 medical device quality management protocols.
- Material Integrity: We utilize exclusively biocompatible, 304 and 316-grade surgical stainless steel, ensuring zero corrosion and maximum tensile yield strength.
- Стерилизация: Every single needle is blister-packed in medical-grade Tyvek and sterilized using Ethylene Oxide (EtO) gas or Gamma Irradiation. Routine biological indicator testing ensures absolute sterility with a guaranteed 5-year shelf life, protecting the hospital’s long-term inventory investments.

VI. Frequently Asked Questions (FAQs)
To assist procurement officers, clinicians, and patients in understanding the nuances of these procedures, we have compiled detailed answers to the industry’s most frequently searched queries.
A biopsy needle works by utilizing specific mechanical actions to extract tissue. A fine aspiration needle works via a vacuum; when the syringe plunger is pulled, negative pressure draws loose cells into the hollow needle. Conversely, a core biopsy needle works via a mechanical shearing action. It features an inner needle with a small notch to catch the tissue, and an outer razor-sharp tube that rapidly slides over the inner needle, cleanly slicing off the trapped tissue and safely holding it inside the needle for removal.
The actual mechanical deployment of the needle—the moment it enters the tumor and extracts the sample—takes only a fraction of a second. However, the comprehensive procedure takes between 15 and 45 minutes. This time includes positioning the patient, sterilizing the skin, administering local anesthesia, utilizing ultrasound or CT imaging to perfectly locate the lesion, and verifying that the extracted samples are adequate before the patient is bandaged.
A 9-gauge needle is considered exceptionally large in the realm of medical needles, featuring an outer diameter of approximately 2.9 millimeters. Because of its large size, it is never used for routine superficial biopsies. It is primarily utilized in Vacuum-Assisted Biopsy (VAB) systems to extract large volumes of breast tissue (often to completely remove small benign fibroadenomas) or in highly specialized bone marrow harvesting procedures.
A Tru-Cut biopsy needle (a semi-automatic or manual core needle) is used in a precise, three-step sequence. First, the physician advances the closed needle assembly through the skin to the very edge of the tumor. Second, the physician manually pushes the inner stylet forward, piercing the tumor and exposing the sample notch so tissue falls into it. Third, the physician pushes the outer cutting cannula rapidly forward over the stylet. This action slices the tissue and locks the sample safely inside the notch so it can be withdrawn from the body.
A core needle biopsy is a definitive diagnostic procedure that uses a specialized, hollow needle to extract a small, intact cylinder (a “core”) of tissue from an abnormal mass. Unlike cytology (which only looks at loose, disorganized cells), a core biopsy preserves the exact architectural structure of the tissue. This allows pathologists to perform a histological examination to accurately grade the severity of a cancer and identify specific molecular markers crucial for targeted chemotherapy.
A needle aspiration biopsy, clinically known as Fine Needle Aspiration Cytology (FNAC), is a minimally invasive diagnostic technique. A physician inserts a very thin, hollow needle (similar to those used for blood draws) into a suspicious lump. Using an attached syringe, the physician creates a vacuum to “aspirate” or suction out individual cells and fluid. These cells are then smeared onto a slide and examined under a microscope to determine if the lump is benign, malignant, or an infectious cyst.
The Silverman biopsy needle is a historical medical instrument invented in the 1930s and was one of the earliest tools used for core tissue biopsies. It featured a unique, longitudinally split inner stylet (like a two-pronged fork) designed to grasp the tumor tissue while an outer cannula sheared it off. While it was highly innovative for its time, it has been almost entirely rendered obsolete and replaced by modern, automated spring-loaded biopsy guns that are faster, safer, and less painful for the patient.
While clinical statistics vary slightly by region and the specific demographic being screened, historically, approximately 20% to 30% of breast biopsies return a positive diagnosis for malignancy (breast cancer). This is a crucial statistic because it means the vast majority of breast biopsies—roughly 70% to 80%—reveal benign (non-cancerous) conditions such as fibroadenomas, cysts, or harmless calcifications. The biopsy is essential not just for finding cancer, but for safely ruling it out.
Bone marrow biopsies require specialized, highly robust needles capable of being manually driven through the hard outer cortex of the pelvic bone (the iliac crest) without bending or breaking. The standard bone marrow biopsy needle size for an adult patient is typically an 8-gauge to 11-gauge needle. For pediatric patients, a slightly smaller 13-gauge needle is typically utilized to accommodate their smaller bone structure while still obtaining an adequate marrow core.