The global landscape of hormonal health has evolved significantly over the last decade. With the rising prevalence of Testosterone Replacement Therapy (TRT) for treating hypogonadism, hormone optimization, and gender-affirming care, millions of patients are navigating the intricacies of self-administered injections.
At the core of a successful TRT protocol are two vital components: the prescribed medication and the medical consumables used to deliver it. Even the most perfectly calibrated dose of testosterone can result in a poor patient experience if administered with suboptimal equipment. Whether a patient or provider chooses the traditional Intramuscular (IM) route or the increasingly popular Subcutaneous (SubQ) route, the goal remains the same: safe, effective, and minimally painful delivery.
In this comprehensive guide, we will explore the nuances of testosterone injection subcutaneous vs intramuscular methods, detail the pharmacological timelines of these treatments, and underscore why utilizing premium-grade syringes and needles is non-negotiable for modern patient care.
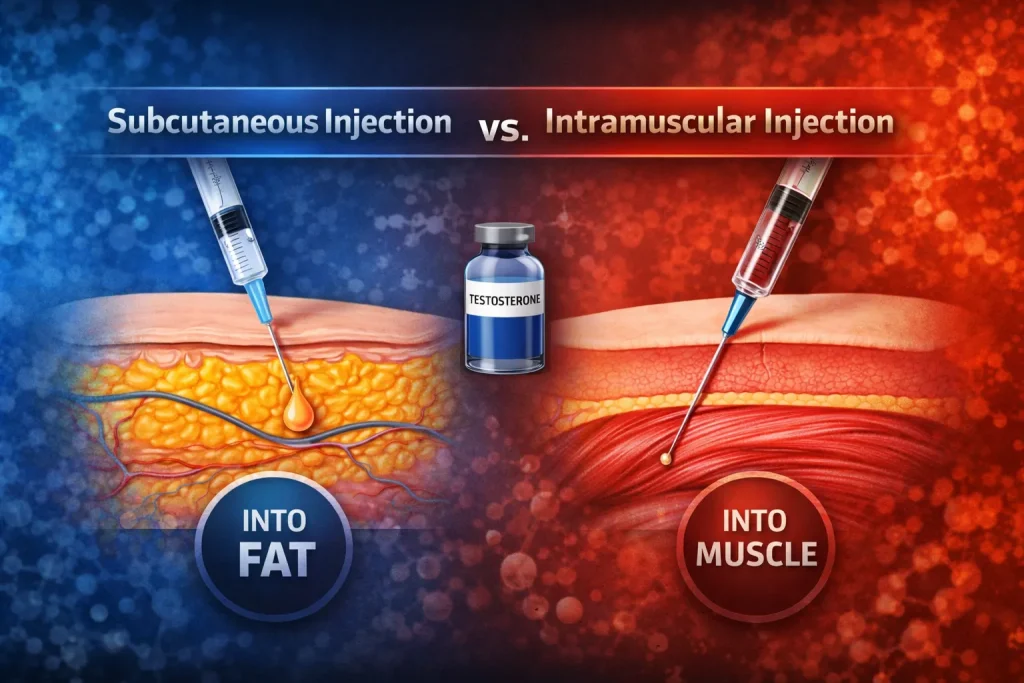
II. Understanding the Basics: Subcutaneous vs. Intramuscular
Testosterone, typically formulated as an ester (like testosterone cypionate or enanthate) suspended in a carrier oil, must be injected into the body to bypass the destructive first-pass metabolism of the liver. The two primary methods for this injection are intramuscular (into the muscle) and subcutaneous (into the fatty tissue just beneath the skin).
Intramuscular (IM) Injections
Historically, IM injections have been the gold standard for TRT. Because muscle tissue has a deep and rich blood supply, medications injected here are absorbed steadily into the bloodstream.
- Common Injection Sites: En vastus lateralis (outer thigh), the ventrogluteal (hip/glute), and occasionally the deltoid (shoulder) for smaller volumes.
- The Pros: IM allows for larger volumes of oil to be injected at once (up to 3mL in large muscles, though TRT doses are usually much smaller). It is a well-established, medically traditional route with decades of pharmacokinetic data supporting its efficacy.
- The Cons: IM injections require longer needles to bypass the subcutaneous fat layer and reach the muscle. This can cause higher anxiety in patients. Furthermore, frequent IM injections can lead to localized muscle trauma, microscarring, and post-injection pain (PIP).
Subcutaneous (SubQ) Injections
Subcutaneous injections deliver the testosterone into the adipose (fat) tissue layer between the skin and the muscle. While once thought unsuitable for oil-based hormones, recent clinical studies have shown SubQ to be highly effective for TRT.
- Common Injection Sites: The lower abdomen (excluding a two-inch radius around the umbilicus), the outer thighs, and the back of the upper arms.
- The Pros: The SubQ route utilizes much shorter, thinner needles, dramatically reducing patient anxiety and injection pain. Because fat tissue has fewer blood vessels than muscle, the absorption rate is often slower and steadier, which can lead to more stable blood serum testosterone levels and lower spikes in estrogen conversion (aromatization).
- The Cons: The SubQ tissue cannot handle large volumes of oil well. Injections of more than 0.5mL subQ can cause small, usually painless, raised lumps under the skin (nodules) that take a few days to absorb.
IM vs. SubQ: An Authoritative Comparison
| Característica | Intramuscular (IM) | Subcutánea (SubQ) |
| Tejido diana | Deep muscle fibers | Adipose (fat) layer beneath skin |
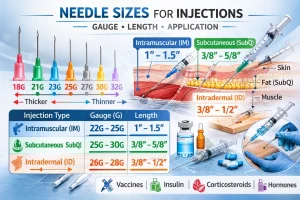
| Typical Needle Length | 1 inch to 1.5 inches | 1/2 inch to 5/8 inch |
| Typical Needle Gauge | 22G - 25G | 25G - 30G |
| Volume Capacity | High (up to 3mL) | Low (Max 0.5mL per site recommended) |
| Absorption Rate | Steady to Fast | Slow and Highly Stable |
| Confort del paciente | Moderate to High PIP risk | High comfort, very low pain |
| Best For | Infrequent, large-dose injections | Frequent, micro-dosing protocols |
III. Selecting the Right Injection Equipment
As a medical consumables manufacturer, we understand that the point of contact—the needle and syringe—dictates the patient’s entire physical experience of TRT. High-quality precision engineering reduces tissue trauma, mitigates pain, and prevents medication waste.
Choosing the Syringe
Testosterone is a viscous (thick) fluid that plays a major role in syringe selection. When determining the best syringe for testosterone injection, you must consider both the volume of the dose and the design of the syringe tip.
- Volume Capacity: Most TRT doses range from 0.2mL to 1mL. Therefore, a 1mL or 3mL syringe is ideal. Using a 1mL syringe allows for incredibly precise measurements, which is crucial for modern micro-dosing protocols.
- Low Dead Space: A standard syringe leaves a tiny amount of medication trapped in the hub after the plunger is pushed all the way down. Over months of weekly injections, this “dead space” results in significant medication waste. Low dead-space syringes are engineered to push nearly 100% of the fluid out, maximizing the use of the prescribed testosterone.
- Luer-Lock Technology: Because oil is thick, it requires pressure to push through a thin needle. Luer-lock syringes, which allow the needle to twist and lock onto the jeringa, prevent the needle from popping off under pressure.
Choosing the Needle
En best needle to inject testosterone depends on whether the patient is drawing the medication from the vial or injecting it into the body.
- Drawing Needles: To draw thick oil from a multi-dose vial efficiently without creating a vacuum, a thicker gauge needle (such as an 18G or 20G) is highly recommended.
- Injecting Needles: Once the medication is in the syringe, the thick drawing needle is swapped for a thinner injecting needle. The ideal injecting needle features surgical-grade stainless steel, a multi-beveled tip for a precision cut (rather than a tear) through the skin, and a medical-grade silicone coating to ensure a smooth glide.
Modern Alternatives: The Auto-Injector
In recent years, the testosterone self-injection pen has entered the market. These devices, similar to EpiPens or insulin pens, are pre-filled and spring-loaded. They are specifically designed for SubQ administration. While they offer unparalleled convenience and completely hide the needle from view (great for needle-phobic patients), they are significantly more expensive and offer less flexibility in dose titration compared to drawing from a standard vial with a high-quality manual syringe.
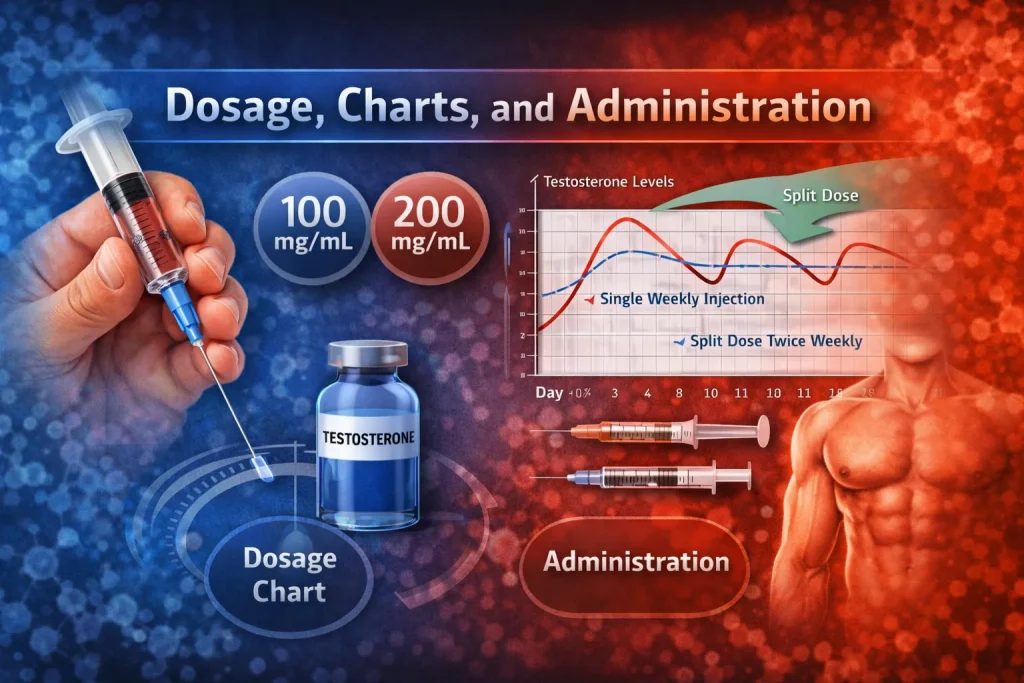
IV. Dosage, Charts, and Administration
Because TRT is a highly individualized therapy, there is no single “correct” dose. Doses are titrated based on comprehensive blood work, the patient’s natural hormone metabolism, and their specific symptom resolution.
Typical Dosage Ranges
For adult males treating hypogonadism, the average dose of testosterone injection generally falls between 100mg and 200mg per week. Traditionally, this was administered as one large IM injection every 7 to 14 days. However, modern endocrinology favors splitting the dose (e.g., 50mg twice a week) to prevent dramatic peaks and valleys in hormone levels.
Reading a Dosage Chart
Understanding a testosterone injection dosage chart is critical for both providers and patients. The concentration of testosterone in the vial dictates how many milliliters (mL) must be drawn into the syringe to achieve the prescribed milligram (mg) dose. The most common concentration for Testosterone Cypionate in the US is 200mg/mL.
Quick Reference Dosage Chart (Based on a 200mg/mL Concentration)
| Prescribed Dose (mg) | Volume to Draw in Syringe (mL or cc) |
| 20 mg | 0.1 mL |
| 40 mg | 0.2 mL |
| 50 mg | 0.25 mL |
| 60 mg | 0,3 ml |
| 80 mg | 0.4 mL |
| 100 mg | 0,5 ml |
| 150 mg | 0.75 mL |
| 200 mg | 1,0 ml |
Considerations for Female Patients
Testosterone is not just a male hormone; it plays a crucial role in female libido, energy, and bone density. However, the female testosterone injection dosage is vastly different. Women generally require only one-tenth to one-twentieth of a standard male dose (often ranging from 1mg to 5mg per week).
Because these doses are incredibly small (e.g., 0.05mL of a 100mg/mL vial), precision is paramount. Women, and transitioning patients requiring micro-doses, must utilize ultra-fine 1mL syringes (often insulin syringes) with clear, distinct gradations to prevent accidental virilization from overdosing.
V. Potential Side Effects and Patient Safety
While TRT is widely considered safe when monitored by a physician, introducing exogenous hormones and injecting oils into the body carries inherent risks.
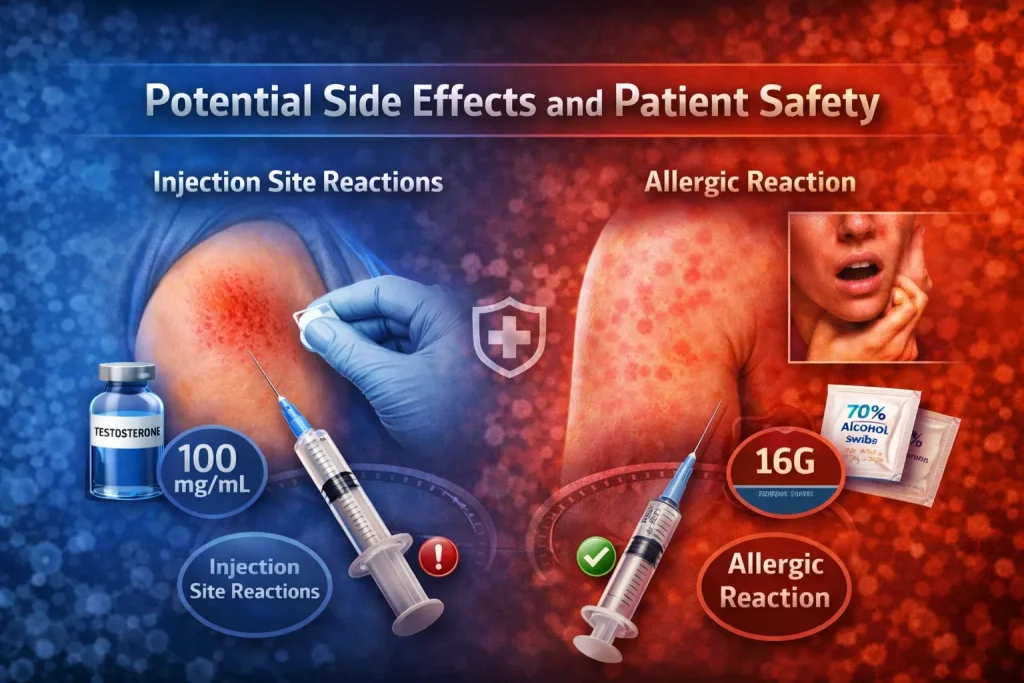
General Injection Site Reactions
The most common side effect is Post-Injection Pain (PIP). This can present as mild bruising, soreness, or redness at the site. Proper technique—such as rotating injection sites, warming the vial slightly before drawing the oil, and injecting slowly—can mitigate these issues. Using premium, sharp needles that do not dull upon skin entry is the most effective way to prevent tissue trauma.
Identifying an Allergic Reaction
True allergies to the synthetic testosterone molecule itself are exceptionally rare. However, an allergic reaction to testosterone injection is usually a reaction to the carrier oil or the preservatives (like benzyl alcohol). Testosterone is commonly suspended in cottonseed oil, grapeseed oil, or sesame oil.
Symptoms of an allergic reaction include:
- Severe, spreading redness or hives around the injection site.
- Intense itching or a rash that spreads beyond the immediate area.
- Swelling of the lips, tongue, or face.
- Shortness of breath (requires immediate emergency medical attention).
If a patient exhibits localized oil allergies, a physician can usually resolve the issue by switching the prescription to a formulation utilizing a different carrier oil.
Infection Prevention
Safety begins with sterility. Patients must be educated on the absolute necessity of using a fresh, sterile, single-use needle and syringe for every injection. Reusing needles microscopically blunts the tip (causing severe pain) and introduces bacteria, leading to dangerous abscesses. Wiping the vial stopper and the injection site with a 70% isopropyl alcohol swab is a mandatory step.
Frequently Asked Questions
Navigating TRT requires specific, actionable knowledge. Below are the most common questions asked by patients regarding equipment, timelines, and expectations.
For the vast majority of TRT patients, a 1mL or 3mL syringe is ideal. If your prescribed dose requires drawing less than 1mL of fluid (e.g., 0.5mL), a 1mL syringe is highly recommended because the tick marks are spaced further apart, allowing for a much more accurate measurement.
Needle size is measured in “gauge” (G). The higher the number, the thinner the needle. Because testosterone is thick, patients commonly use an 18G or 20G needle to draw the medication from the vial. For the actual injection, a 23G to 25G needle is standard for Intramuscular (IM), while a 25G to 27G needle is preferred for Subcutaneous (SubQ).
Always look for a “Luer-Lock” syringe. Because you are pushing a viscous oil through a very thin needle, the pressure inside the syringe builds up. A Luer-Lock syringe features threads that lock the needle into place, preventing it from blowing off during the injection. Low dead-space variants are also recommended to save medication.
Testosterone Cypionate is frequently suspended in cottonseed oil, which is notably thick. While you still want a thin needle for comfort, going too thin (like a 29G or 30G insulin needle) can make pushing the Cypionate oil very difficult and time-consuming. A 25G needle represents the perfect “sweet spot” for Cypionate—thin enough to be relatively painless, but wide enough to allow the thick oil to flow steadily.
Needle length depends entirely on your chosen injection method and your body composition.
For IM injections: A 1-inch to 1.5-inch needle is required to penetrate through the skin and fat layer into the deep muscle.
For SubQ injections: A 1/2-inch or 5/8-inch needle is ideal to ensure the medication is deposited safely in the fat layer without accidentally hitting the muscle below.
Biologically, the body begins absorbing the hormone immediately. However, physically and mentally, you will likely not feel anything profound right away. Some patients report a mild “placebo” boost in energy or a slight warmth, but actual physiological changes take time. You may experience mild soreness at the injection site a day later.
Pharmacokinetically, a standard injection of Testosterone Cypionate reaches its maximum concentration (the “peak” in your bloodstream) approximately 48 to 72 hours after the injection. From that point, levels gradually decline (the “trough”) until the next scheduled dose.
When monitoring TRT, endocrinologists generally want to see your “trough” levels—the lowest point your testosterone reaches. Therefore, you should schedule your bloodwork on the morning of your injection day, before you take your shot. If you inject on Monday mornings, get your blood drawn early Monday morning before injecting.
If you are treating clinical hypogonadism (low T), the initial relief of symptoms—such as an improvement in brain fog, slight increases in morning energy, and a bump in libido—usually begins to become noticeable between weeks 3 and 6 of consistent injections.
The effects of TRT are cumulative. While libido and energy may improve in the first month, structural changes take much longer. Improvements in muscle mass and fat distribution typically take 3 to 6 months to become apparent. Maximum improvements in bone mineral density can take upwards of 12 to 24 months of consistent therapy.
VII. Conclusión
Whether a patient and their healthcare provider decide on the deeper penetration of an Intramuscular route or the stable, low-pain profile of Subcutaneous administration, the mechanics of a successful TRT regimen rely heavily on the tools used. Understanding proper dosages, the pharmacokinetics of the hormone, and adhering strictly to sterile protocols ensures patient safety and optimal therapeutic outcomes.
At the heart of this process are the needles and syringes. Supplying patients with high-quality, precision-engineered medical consumables is not just about convenience; it is about minimizing trauma, eliminating medication waste, and ensuring that a life-changing therapy isn’t hindered by subpar equipment.